Compensatory Responses to Heart Failure
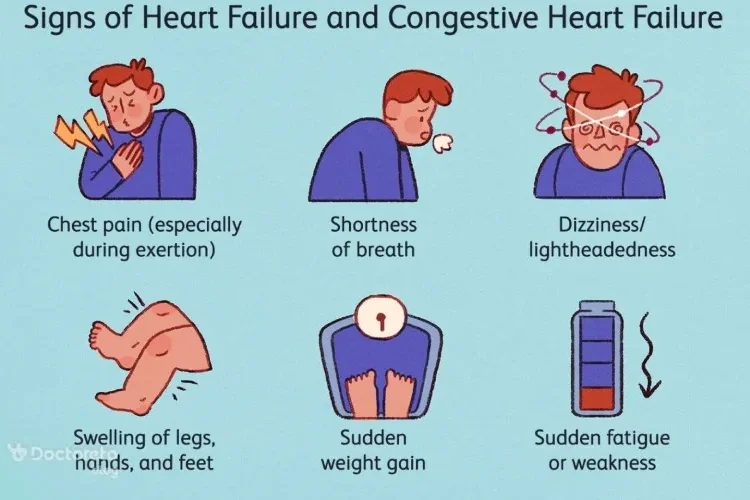
Heart failure (HF) is a progressive disorder that heart is unable to pump sufficient blood to for the needs of the body. HF is because of an impaired ability of the heart to adequately fill with and/or eject blood. It’s often accompanied by abnormal increase in interstitial fluid and blood volume. Underlying causes of HF are atherosclerotic heart disease, hypertensive heart disease, valvular heart disease, and congenital heart disease. Symptoms include:
- Chest pain specially during exertion
- Shortness of breath (dyspnea)
- Dizziness/ Light-headedness
- Swelling of legs, hands and feet (fluid retention)
- Sudden weight gain
- fatigue or weakness
There are some compensatory responses to heart failure that should not stay untreated. Chronic activation of the sympathetic nervous system and the renin- angiotensin- aldosterone system (RAAS) is associated with remodeling of cardiac tissue, loss of myocytes, hypertrophy, and fibrosis. This causes additional neurohormonal activation, creating a vicious cycle that can lead to death if left untreated. In this context we are going to assess these compensatory responses, and their effects on body.
1. Increased sympathetic activity:
Baroreceptors sense blood pressure decrease and activate sympathetic nervous system. Beta adrenergic receptors stimulation results in increased heart rate and a greater force of heart muscle contraction. Vasoconstriction enhances venous return and increases cardiac preload, so then we have cardiac output increase. This response increases heart workload, but by the time it will have bad effects on cardiac function.
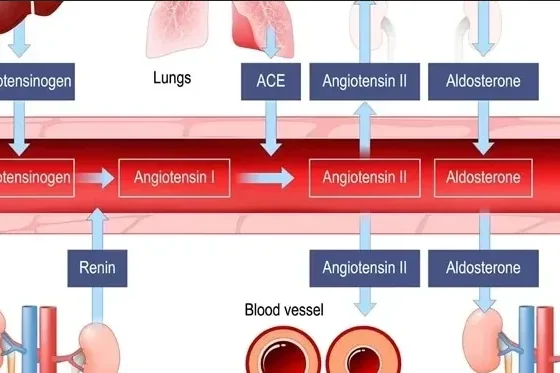
2. Activation of the renin- angiotensin- aldosterone system (RAAS)
A fall in cardiac output decreases blood flow to the kidney, so it causes the release of renin. Increased formation of angiotensin II and aldosterone release also stimulates renin release. This results in increased peripheral resistance (afterload) and sodium and water retention. Then blood volume increases, and this more blood return to the heart. If the heart can’t pump this extra volume, venous pressure increases and peripheral and pulmonary edema occur. When angiotensin II and aldosterone increase, detrimental effects can happen for cardiac muscle, favoring remodeling, fibrosis, and inflammatory changes. These responses increase heart workload, so cardiac function decreases as time passes.
1. Increased sympathetic activity:
Baroreceptors sense blood pressure decrease and activate sympathetic nervous system. Beta adrenergic receptors stimulation results in increased heart rate and a greater force of heart muscle contraction. Vasoconstriction enhances venous return and increases cardiac preload, so then we have cardiac output increase. This response increases heart workload, but by the time it will have bad effects on cardiac function.
2. Activation of the renin- angiotensin- aldosterone system (RAAS)
A fall in cardiac output decreases blood flow to the kidney, so it causes the release of renin. Increased formation of angiotensin II and aldosterone release also stimulates renin release. This results in increased peripheral resistance (afterload) and sodium and water retention. Then blood volume increases, and this more blood return to the heart. If the heart can’t pump this extra volume, venous pressure increases and peripheral and pulmonary edema occur. When angiotensin II and aldosterone increase, detrimental effects can happen for cardiac muscle, favoring remodeling, fibrosis, and inflammatory changes. These responses increase heart workload, so cardiac function decreases as time passes.
3. Activation of natriuretic peptides:
An increase in preload increases the release of natriuretic peptides. Atrial, B-type and C-type natriuretic peptides are in our body. Natriuretic peptides activation ultimately results in vasodilation, natriuresis, inhibition of renin and aldosterone release, and reduction in myocardial fibrosis. This response may improve cardiac function and heart failure symptoms.
4. Myocardial hypertrophy:
Stretching of the heart muscle leads to a stronger contraction of the heart. However, excessive elongation of the fibers results in weaker contractions and a diminished ability to eject blood. We call this type of failure, “systolic failure” or “heart failure with reduced ejection fraction” (HFrEF) and it’s because of ventricle being unable to pump effectively. HF can be also as diastolic dysfunction that happens when the ability of ventricles to relax and accept blood is impaired by structural changes such as hypertrophy. In this case, ventricles’ wall become thick and we have decrease in ventricular volume, so heart muscle has less ability to relax, and ventricles doesn’t fill adequately. We call this one diastolic HF or HF with preserved ejection fraction (HFpEF). Diastolic dysfunction is characterized by signs of HF in the presence of a normal functioning left ventricle. However, both systolic and diastolic dysfunction commonly coexist in HF.
An increase in preload increases the release of natriuretic peptides. Atrial, B-type and C-type natriuretic peptides are in our body. Natriuretic peptides activation ultimately results in vasodilation, natriuresis, inhibition of renin and aldosterone release, and reduction in myocardial fibrosis. This response may improve cardiac function and heart failure symptoms.
4. Myocardial hypertrophy:
Stretching of the heart muscle leads to a stronger contraction of the heart. However, excessive elongation of the fibers results in weaker contractions and a diminished ability to eject blood. We call this type of failure, “systolic failure” or “heart failure with reduced ejection fraction” (HFrEF) and it’s because of ventricle being unable to pump effectively. HF can be also as diastolic dysfunction that happens when the ability of ventricles to relax and accept blood is impaired by structural changes such as hypertrophy. In this case, ventricles’ wall become thick and we have decrease in ventricular volume, so heart muscle has less ability to relax, and ventricles doesn’t fill adequately. We call this one diastolic HF or HF with preserved ejection fraction (HFpEF). Diastolic dysfunction is characterized by signs of HF in the presence of a normal functioning left ventricle. However, both systolic and diastolic dysfunction commonly coexist in HF.